

Introduction
The mention of the Ebola virus is often accompanied by public fear and ignorance. Classified as a Biosafety Level 4 (BSL-4) pathogen, it has long ranked among the world’s most dangerous viruses due to its extremely high fatality rate and characteristic hemorrhagic symptoms, despite not triggering large-scale global pandemics. Recently, multiple African countries have reported new confirmed Ebola cases, prompting the World Health Organization (WHO) to launch an emergency response mechanism. Faced with this hidden and lethal killer, panic is futile, and scientific cognition serves as the best line of defense. This article systematically elaborates on the biological characteristics of the Ebola virus and its pathogenic mechanism in humans, and deeply analyzes the core principles of antigen and antibody detection, enabling a comprehensive understanding of the scientific methods to combat Ebola.
Understanding the Pathogen: The Immune Evasion Camouflage of Filoviruses
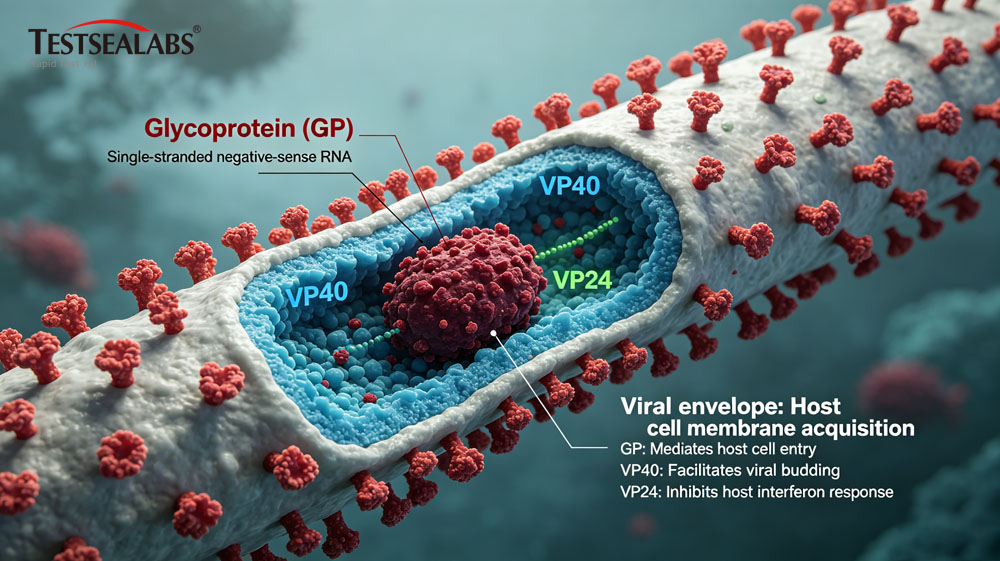
The Ebola virus belongs to the Filoviridae family. Under an electron microscope, it presents unique morphologies including curved filaments, U-shapes and “6″ shapes, with a maximum length of 14,000 nanometers, far larger than influenza viruses. The virus has a single-stranded negative-sense RNA core of approximately 19kb, encoding 7 structural proteins, among which three core proteins are critical for its pathogenicity and immune evasion.
Glycoprotein (GP) is distributed on the virus surface to form spike structures, acting as the core carrier for the virus to bind to host cell receptors. It can simulate benign human signals to interfere with immune recognition and achieve effective camouflage. Matrix proteins VP40 and VP24 are mainly responsible for virus assembly and proliferation, while strongly inhibiting host interferon immune responses. In particular, VP24 directly blocks the interferon signal transduction pathway, allowing the virus to replicate silently and invade stealthily in the early stage of infection, greatly weakening the human body’s first line of immune defense. This constitutes the core reason for the Ebola virus’s powerful immune evasion capability.
Chain: From Fruit Bat Reservoirs to Human-to-Human Spread
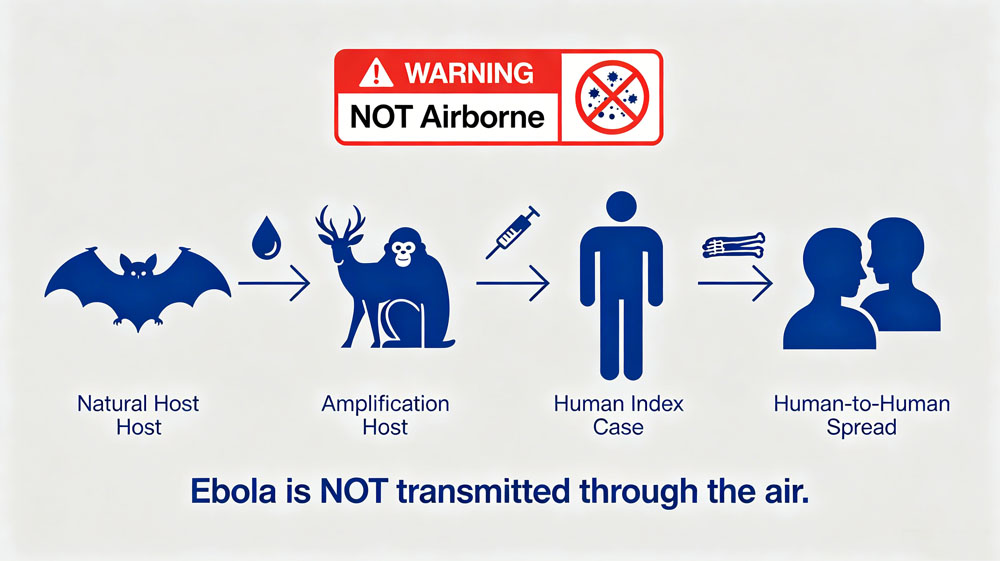
A large number of epidemiological studies have confirmed that African fruit bats such as hammer-headed fruit bats and little collared fruit bats are natural reservoir hosts of the Ebola virus. These bats carry the virus without developing symptoms and release it into the natural environment through saliva and feces. Most primary human infections stem from zoonotic spillover events, where humans come into contact with virus-infected wild animals including chimpanzees, gorillas, antelopes and porcupines, enabling cross-species transmission of the virus from animals to humans.
After successfully infecting humans, the virus spreads rapidly through close human-to-human contact. Human body fluids such as blood, vomit, feces, urine, saliva, semen and breast milk are high-risk sources of infection. Infection may occur when damaged skin or mucous membranes of the eyes, mouth and nose come into contact with virus-contaminated items such as bed sheets and medical devices. Notably, deceased bodies are highly contagious during funeral handling, as the virus can survive for several days in corpses, posing a major hidden danger for epidemic transmission.
Core Fact Check: The Ebola virus is not airborne. It cannot achieve long-distance human-to-human transmission via aerosol droplet nuclei suspended in the air. Infection is only possible at extremely close distances when virus-laden body fluid droplets splash directly onto human mucous membranes, which does not constitute typical airborne transmission. Therefore, as long as direct contact with body fluids is avoided and standard personal protection is implemented, the infection risk in daily public scenarios is extremely low.
Progression: From Early Fever to Lethal Cytokine Storm
The incubation period of Ebola virus infection ranges from 2 to 21 days, with an average of 8 to 10 days, and the virus is non-contagious during incubation. The disease progresses rapidly after onset, divided into three typical progressive stages, with severe patients quickly developing multi-organ failure.
The first stage is the non-specific febrile phase (Days 1-3 after onset). Patients develop sudden high fever above 38.5℃, accompanied by severe headache, generalized arthralgia and myalgia, sore throat and extreme fatigue. The clinical manifestations are highly overlapping with influenza, malaria and typhoid fever with no specific features, which is the main cause of early clinical missed and misdiagnosis.
The second stage is the gastrointestinal and vascular damage phase (Days 4-7 after onset). Patients suffer from persistent vomiting, watery diarrhea and severe abdominal pain, which easily lead to severe dehydration and electrolyte disorders. Meanwhile, the virus targets and attacks vascular endothelial cells, destroys capillary integrity, induces coagulation disorders, and causes symptoms such as gingival bleeding, epistaxis, pinhole oozing and conjunctival congestion. Approximately half of patients develop systemic internal and external bleeding, including hematemesis, hematochezia and visceral hemorrhage.
The third stage is the terminal or recovery phase (Day 8 and after onset). If the human immune system fails to effectively suppress viral replication, patients will rapidly develop septic shock and multi-organ failure, with most deaths occurring 6 to 16 days after onset. High viral loads can be detected in all systemic tissues (including eyeballs, testes and placentas) of deceased patients. If the immune system initiates an effective response, patients’ symptoms gradually alleviate 7 to 10 days after onset, yet the recovery period is lengthy. Some survivors have persistent residual virus in their bodies, with detectable virus in semen for up to 18 months, requiring long-term protective measures.
Core Value of Testing: Diagnosis Relies Solely on Detection Rather Than Symptoms
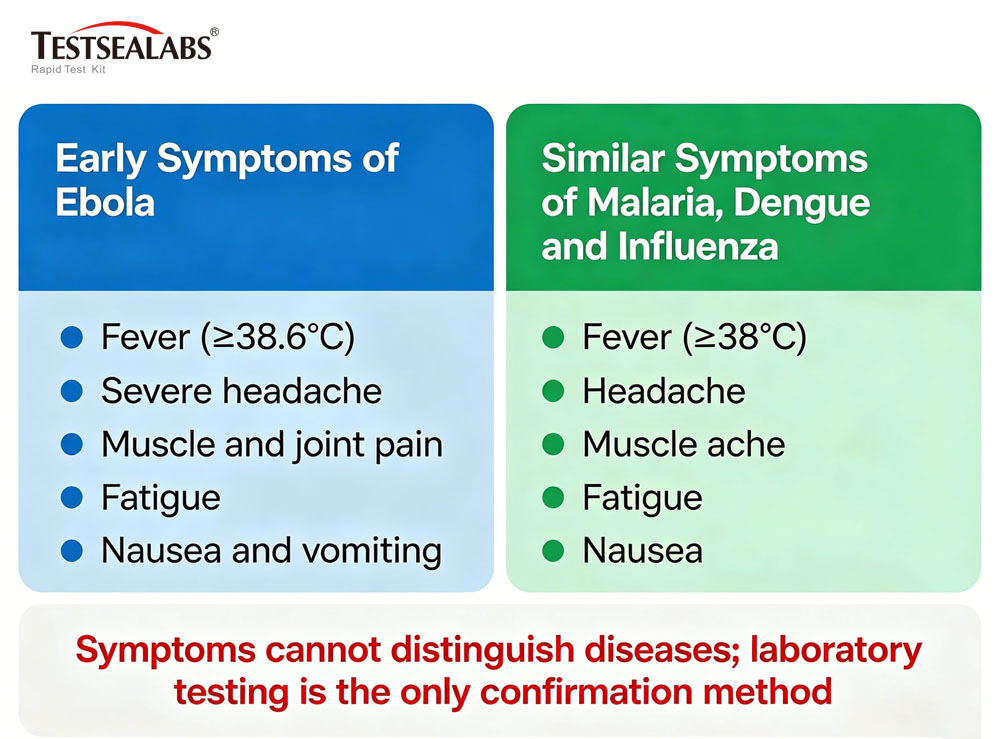
As indicated by the disease progression characteristics, early symptoms of Ebola infection are non-specific. In high-prevalence African regions, infectious diseases such as malaria, dengue fever, Lassa fever and yellow fever are endemic simultaneously, making clinical differentiation impossible based solely on symptoms. Without laboratory testing support, two major risks will inevitably arise: first, suspected Ebola patients admitted to general wards may cause nosocomial cluster infections and epidemic spread; second, patients with common infectious diseases may be misdiagnosed and isolated as Ebola cases, resulting in wasted medical resources and delayed optimal treatment for conventional illnesses.
Therefore, rapid and accurate laboratory testing is the cornerstone of Ebola epidemic prevention and control. The WHO recommends three mainstream detection technologies: nucleic acid PCR testing, antigen testing and antibody testing. Based on mature immunological principles, antigen and antibody testing feature simple operation and strong adaptability, serving as core detection methods for on-site epidemic response and grassroots prevention and control.
Antigen Detection: Directly Capturing Viral Invasion Traces
Antigens are specific substances that can be recognized by the human immune system and trigger immune responses. For the Ebola virus, its surface glycoprotein (GP) and internal nucleoprotein (NP) are core specific antigens, equivalent to the unique “identity barcode” of the virus and the key targets for detection and identification.
Currently, the commonly used rapid Ebola antigen detection in clinical and on-site scenarios adopts the immunochromatographic method, consistent with the principle of COVID-19 antigen test strips, with the core being the double-antibody sandwich method featuring simple and efficient operation. Patient samples of blood, saliva or urine are dropped onto the test strip sample pad and permeate forward via capillary action. If Ebola virus antigens exist in the sample, they will bind to the nano-gold labeled antibodies on the strip to form antibody-antigen complexes. The complexes migrate to the test line (T line), where they are captured and enriched by fixed antibodies to develop color; the remaining liquid flows through the control line (C line) to verify the validity of the test strip.
Result interpretation criteria: color development on both C line and T line indicates positive, suggesting viral infection; color development only on the C line indicates negative with no virus detected; no color development on the C line means the test strip is invalid and the result is ineffective.
This detection technology has remarkable advantages: results are available within 15 to 30 minutes, no sophisticated large-scale equipment is required, and test strips can be stored at room temperature for short-term use, suitable for rapid screening in grassroots medical institutions and remote epidemic areas. However, it has limitations with lower sensitivity than nucleic acid PCR testing, only detecting samples with high viral loads (Ct value < 35), and prone to false negatives when the viral load is low within 1 to 3 days after onset. At present, the WHO has approved rapid antigen testing as an official diagnosis basis in remote areas without PCR detection conditions for rapid epidemic screening and case confirmation.
Antibody Detection: Tracing the Immune Combat Traces of the Human Body
Antibodies are specific Y-shaped immunoglobulins produced by human B lymphocytes stimulated by viral antigens, with a unique “lock-and-key matching” binding property that only recognizes a single pathogen. After Ebola virus infection, the human body sequentially produces two types of core protective antibodies, which accurately reflect the infection stage and immune status.
IgM antibodies are produced 7 to 10 days after infection and peak within 2 to 4 weeks, serving as core markers of recent acute infection. IgG antibodies emerge later, gradually forming 14 to 21 days after infection and persisting in the body for years or even decades, acting as important evidence of previous infection and immune protection.
Enzyme-Linked Immunosorbent Assay (ELISA) is currently the gold standard for antibody detection. The core procedure is as follows: recombinant Ebola antigens are coated at the bottom of microplates, and diluted patient serum is added. If corresponding antibodies exist in the serum, they will bind specifically to the antigens. After washing to remove unbound impurities, enzyme-labeled anti-human antibodies are added. Following a second wash, substrates are added for color development, and the color depth is positively correlated with serum antibody concentration, enabling accurate determination of antibody levels.
It is important to note that antibody detection cannot be used for early diagnosis. Specific antibodies have not been synthesized in the early stage of infection, so negative antibody results cannot rule out infection. This technology is mainly applied in four scenarios: epidemiological traceability investigation, diagnosis of convalescent patients, evaluation of vaccine immune efficacy, and screening of donors for convalescent plasma therapy.
Key Factors Affecting Detection Results
First, sampling time. The viral load is extremely low within 2 days after onset, leading to frequent false negatives in nucleic acid and antigen testing. Clinical recommendations suggest sampling 3 days after fever onset for higher accuracy. Second, sample type. Whole blood and serum are the optimal detection samples, while saliva and urine have low viral content with relatively insufficient detection sensitivity. Third, viral variation. The Ebola virus RNA polymerase lacks proofreading function and is prone to gene mutations, yet the mainstream detection targets are highly conserved nucleoprotein gene regions, enabling existing detection reagents to effectively identify variant strains without large-scale failure. Fourth, biosafety operation. All virus samples must be processed in BSL-2 or higher-level laboratories, and operators must wear full protective equipment to avoid occupational exposure risks.
Authoritative Answers to Public Frequently Asked Questions
1.Will I be infected by an adjacent passenger when taking public transport such as airplanes?
No. Ebola only spreads through direct contact with virus-laden body fluids. There is no infection risk without body fluid contact during daily social interactions, shared transportation or use of public facilities.
2. Are Ebola survivors still contagious?
There is a limited transmission risk. The virus can persist in survivors’ semen for 18 months and hide in aqueous humor, the central nervous system and placental tissues. The WHO clearly recommends that survivors maintain abstinence or consistent condom use for at least 12 months, with no transmission risk in daily contact.
3. Are there effective vaccines available?
Licensed and effective vaccines are available. The rVSV-ZEBOV recombinant vector vaccine was approved by the European Medicines Agency in 2019, with a clinical trial protective efficacy of 97.5%-100%. Adopting a ring vaccination strategy for emergency vaccination of close contacts of confirmed cases, it can quickly block transmission chains. Currently, it is only used for emergency prevention and control in high-risk epidemic areas rather than universal vaccination.
4. Are there specific drugs for Ebola?
Specific therapeutic drugs are available. Two monoclonal antibody combination drugs, Inmazeb and Ebanga, have been approved by the U.S. FDA, reducing the Ebola fatality rate from over 50% to 35%-40%, with further mortality reduction via early standardized treatment. Meanwhile, intensive supportive care including fluid resuscitation, acid-base correction, oxygenation maintenance, secondary infection control and electrolyte disorder correction is the core foundation of clinical treatment.
5. What should I do if I develop a fever after returning from epidemic areas?
Take the initiative to truthfully declare your travel and contact history in epidemic areas upon entry without concealment. Seek medical treatment at formal medical institutions immediately and inform them of your travel history. The medical institution will conduct dual PCR and antigen testing at the earliest opportunity and arrange observation in a negative-pressure isolation ward until infection is ruled out. Avoid visiting crowded general outpatient departments to prevent potential transmission risks.
Conclusion: Eliminate Fear with Science, Consolidate Defenses with Cognition
Although the Ebola virus is dangerous and lethal, it is not invincible. Over the past four decades, human understanding of Ebola has evolved from scratch to thorough comprehension, and prevention and control methods have developed from nonexistent to mature. A complete prevention and control system covering vaccine prevention, drug treatment, precise detection and scientific protection has now been established. Antigen detection rapidly screens for viral traces, antibody detection records immune marks, and nucleic acid detection safeguards the bottom line of case confirmation. Multiple technologies jointly build a solid scientific defense against the “African Reaper”.
For the public, the ultimate weapon against viruses has never been panic, but scientific rationality. Understanding viral transmission rules and detection principles enables us to stay sober amid rumors and standardize protection and cooperate actively with prevention and control when facing potential risks.
Core Science Summary: Ebola virus is not airborne and is preventable and controllable; early symptoms are non-specific, and laboratory testing is the only basis for confirmed diagnosis; antigen testing is suitable for rapid screening, antibody testing for retrospective evaluation, and nucleic acid testing serves as the gold standard for diagnosis.
References: 2024 Ebola Virus Disease Fact Sheet by the World Health Organization (WHO), CDC Laboratory Diagnostic Guidelines, relevant reviews from The Lancet Infectious Diseases. This article is for popular science dissemination only, and epidemic disposal shall comply with official instructions of local health authorities.
Post time: May-29-2026