
Testsealabs malaria rapid diagnostic test — the tri-line RDT format that can detect P. vivax alongside P. falciparum for comprehensive malaria screening.
When malaria is mentioned in the context of sub-Saharan Africa, the conversation almost always centers on Plasmodium falciparum — the species responsible for the vast majority of severe malaria cases and nearly all malaria-related deaths on the continent. This focus is clinically justified. But it has created a dangerous blind spot: Plasmodium vivax, long dismissed as a minor player in Africa’s malaria landscape, is significantly more prevalent across the continent than most diagnostic programs account for, and the consequences of missing it are measurable in treatment failures and preventable relapses.
For distributors supplying malaria rapid diagnostic tests to public health programs across sub-Saharan Africa, the P. vivax blind spot presents both a clinical challenge and a commercial opportunity. The standard single-band RDTs that dominate procurement across the continent detect P. falciparum-specific HRP-II antigen but do not differentiate P. vivax infections. As a result, patients infected with P. vivax are either misclassified as P. falciparum or — in cases where the test only detects HRP-II — may test negative despite having a clinically significant parasitemia. A tri-line RDT that simultaneously detects P. falciparum, P. vivax, and pan-Plasmodium antigens solves this diagnostic gap in a single test cassette.
As the International Sales Director at Testsealabs, I have spent the past decade working with malaria diagnostic programs across Africa. The P. vivax problem is real, it is growing, and it is under-recognized by the very procurement systems that should be addressing it. This article explains why, and what distributors can do about it.
How P. vivax Became Africa’s Neglected Malaria Species
The conventional wisdom in malaria epidemiology has long held that P. falciparum accounts for more than 95% of malaria cases in sub-Saharan Africa, with P. vivax concentrated in the Horn of Africa — Ethiopia, Somalia, Sudan, and Djibouti — and parts of Southern Africa. This narrative was reinforced by decades of microscopy-based surveillance that struggled to distinguish P. vivax from P. ovale and other non-falciparum species, particularly in low-transmission settings where parasitemia levels are low.
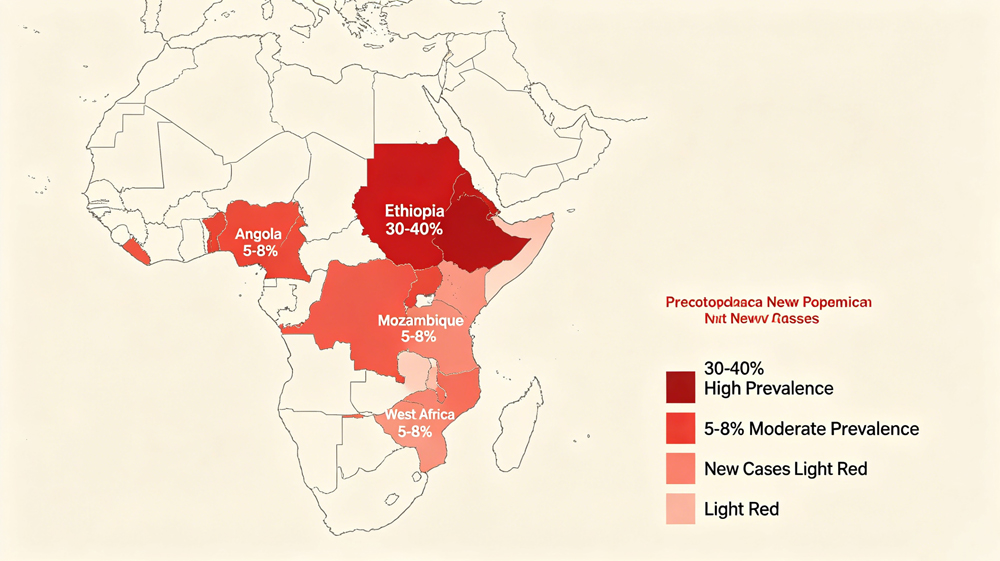
However, recent molecular epidemiological studies — using PCR-based species identification rather than microscopy — have consistently found P. vivax prevalence rates of 5–15% in countries where it was previously thought to be rare or absent. Studies from Ethiopia have documented P. vivax accounting for 30–40% of confirmed malaria cases in certain regions. Reports from Angola, Zambia, Mozambique, and even West African countries like Senegal have identified P. vivax transmission in areas where standard RDT programs would miss it entirely because they rely on falciparum-specific tests.
The clinical implications are significant. Unlike P. falciparum, P. vivax forms dormant liver-stage hypnozoites that can reactivate weeks or months after the initial infection, causing relapses. Treating a P. vivax infection with artemisinin-based combination therapy alone — the standard treatment for uncomplicated P. falciparum — does not eliminate the liver-stage parasites. Without primaquine or tafenoquine for radical cure, the patient remains at risk of relapse. A healthcare worker who diagnoses “malaria” without knowing the species is treating only the acute symptoms, not the root infection.
Country-Level Evidence: Where P. vivax Is Being Missed Across Africa
To understand the scale of the P. vivax underdiagnosis problem, it is worth examining the epidemiological evidence from individual African countries where recent molecular surveillance data has challenged the established narrative:
Ethiopia. Ethiopia has the highest P. vivax burden in Africa, with the species accounting for 30-40% of confirmed malaria cases nationally. In the Amhara and Oromia regions particularly, P. vivax transmission occurs year-round, with seasonal peaks that partially overlap with P. falciparum transmission but also extend beyond it. Despite this established prevalence, the national malaria diagnostic program has historically relied on HRP-II-based RDTs that detect P. falciparum only. The consequence is that patients presenting with P. vivax malaria in health posts that use falciparum-only RDTs receive either no diagnosis (if the test is negative) or a presumptive diagnosis of “clinical malaria” without species confirmation. The WHO’s Global Malaria Programme has specifically highlighted Ethiopia as a country where p.f/p.v dual-species RDTs would improve diagnostic accuracy and treatment outcomes.
Angola and Mozambique. In Southern Africa, molecular surveillance studies conducted in Angola have detected P. vivax in 5-8% of febrile patients presenting to primary health facilities — a rate significantly higher than previously estimated. In Mozambique, studies in the Maputo province have identified focal P. vivax transmission in peri-urban areas. The malaria control programs in both countries use predominantly HRP-II-based RDTs procured through large-scale public health tenders. The presence of P. vivax in these settings means that a proportion of test-negative febrile patients may actually have vivax malaria that is not detected by the available diagnostic tools.
West Africa. P. vivax has historically been considered rare or absent in West Africa due to the high prevalence of the Duffy-negative phenotype — a genetic trait that confers resistance to P. vivax blood-stage infection — in the indigenous populations of the region. However, recent studies from Senegal and Mauritania have documented P. vivax infections in Duffy-positive individuals, suggesting that the parasite is circulating in populations where it was previously not expected. This finding has significant implications for malaria elimination programs in the region, which may need to account for a P. vivax reservoir that existing diagnostic protocols are not designed to detect.
The Horn of Africa. Beyond Ethiopia, Djibouti, Somalia, Sudan, and South Sudan all have documented P. vivax transmission at varying levels of intensity. The movement of populations across borders in this region — including refugees, pastoralists, and seasonal agricultural workers — creates opportunities for P. vivax strains to move between areas with different diagnostic capacities. A P. vivax infection acquired in one country may present clinically in another country where the diagnostic tools in use are falciparum-only, ensuring that the infection is not identified at the species level.
For procurement officers designing malaria diagnostic strategies for these countries, the implication is clear: the assumption that falciparum-only RDTs are sufficient for the national malaria program is no longer supported by the available epidemiological evidence. A p.f/p.v tri-line test provides species-level diagnostic information that improves both individual patient management and the quality of surveillance data. A procurement officer who transitions from falciparum-only to p.f/p.v tri-line RDTs is making an investment in diagnostic accuracy that directly supports the malaria elimination goals that WHO and national malaria control programs have set for the region.
The Hypnozoite Problem: Why Species Differentiation Changes Treatment
The biology of P. vivax sets it apart from P. falciparum in a way that directly affects diagnostic and treatment protocols. When a person is bitten by an Anopheles mosquito carrying P. vivax sporozoites, the parasites travel to the liver and invade hepatocytes. In the liver, some of the parasites immediately develop into schizonts that will go on to infect red blood cells, but a portion develop into hypnozoites — dormant forms that can persist in the liver for weeks, months, or even years before reactivating.
This dormant stage means that a patient who appears to recover from acute P. vivax malaria after ACT treatment may suffer a full-blown relapse weeks later. In areas where P. vivax is endemic, relapses account for a substantial proportion of total clinical episodes. For malaria control programs trying to reduce transmission, failing to diagnose and radically cure P. vivax infections means the parasite reservoir persists in the human population — and the relapse cycle continues.
The WHO guidelines for P. vivax treatment recommend a 14-day course of primaquine for radical cure of the liver stage, in addition to ACT for the acute blood-stage infection. However, this treatment protocol is only appropriate if the clinician knows the patient has P. vivax. An RDT that reports “malaria positive” without species information does not provide the diagnostic discrimination needed for species-appropriate treatment.
The Testsealabs Malaria p.f/p.v Tri-Line Test Cassette addresses this clinical gap directly. The test simultaneously detects P. falciparum-specific HRP-II, P. vivax-specific LDH, and pan-Plasmodium LDH on three separate test lines, providing unambiguous species-level identification within 15 minutes. For a clinician managing a febrile patient in a setting where both P. falciparum and P. vivax are circulating, this diagnostic discrimination changes treatment decisions.
The Procurement Paradox: Why Public Health Programs Miss P. vivax
Given that P. vivax is a clinically significant, treatable, and preventable cause of malaria in Africa, why do public health procurement programs continue to favor falciparum-only RDTs? The answer lies in a combination of historical procurement patterns, cost considerations, and surveillance gaps that create a circular logic problem.
Cost-driven procurement. Single-band HRP-II tests are the lowest-cost option in the malaria RDT market. For procurement officers managing tight budgets, the per-test price difference between a falciparum-only test and a p.f/p.v tri-line test is a visible cost that must be justified. The invisible cost — treatment failures due to P. vivax misdiagnosis, relapse episodes that consume additional healthcare resources, and the ongoing transmission reservoir — is spread across multiple budget lines and rarely appears in the procurement officer’s cost analysis.
Surveillance data that reinforces the blind spot. National malaria surveillance systems report confirmed malaria cases based on the RDTs that are procured. If a country procures only falciparum-specific RDTs, its surveillance system will report 100% of confirmed cases as P. falciparum — which then reinforces the perception that P. vivax is not present, which in turn justifies continued procurement of falciparum-only tests. This circular logic can persist for years, masking the true species distribution.
WHO prequalification inertia. The WHO malaria RDT product testing program has historically focused on P. falciparum detection performance, reflecting the disease burden distribution. While the program has expanded to include P. vivax detection in recent evaluation rounds, the installed base of falciparum-only products in supply chains across Africa remains vast. Transitioning a national program from single-species to dual-species RDTs requires policy change, retraining, and budget reallocation — all of which take time.
Why Distributors Should Add a p.f/p.v Tri-Line RDT to Their Portfolio
For distributors serving the African malaria diagnostic market, adding a quality-assured p.f/p.v tri-line RDT to the product portfolio offers several strategic advantages:
Differentiation in a commodity market. The falciparum-only RDT market is highly commoditized, with dozens of manufacturers competing primarily on price. A tri-line p.f/p.v test that provides species-level differentiation is a genuinely differentiated product — one that distributors can position as a clinical upgrade rather than a commodity replacement.
Alignment with evolving WHO guidance. As molecular surveillance data continues to reveal higher-than-expected P. vivax prevalence across Africa, WHO guidance on diagnostic strategy is likely to evolve toward broader species coverage. Distributors who proactively add p.f/p.v RDTs to their portfolio are positioned ahead of this policy shift rather than scrambling to catch up when it arrives.
Portfolio completeness for febrile illness panels. For distributors offering a comprehensive febrile illness diagnostic portfolio — including malaria, dengue, typhoid, leptospirosis, and other tests — adding a p.f/p.v malaria test that provides species-level information creates a more complete diagnostic offering for clinicians managing undifferentiated febrile patients.
Premium positioning in private healthcare. While public health procurement decisions are driven by cost-per-test, private healthcare providers — including private hospitals, clinics, and corporate occupational health programs — are willing to pay a premium for tests that provide more clinical information. A p.f/p.v tri-line test can be positioned as a premium product for the private healthcare channel.
For a complete view of our malaria RDT range, I encourage distributors to review the Testsealabs Malaria Ag P.f/P.v/Pan Combo Test and our broader infectious disease diagnostics product line.
Real-World Performance: What Heat-Stability Data Tells Us
Beyond the performance specifications on paper, distributors and procurement officers should also consider the real-world implications of species-level RDT differentiation for malaria case management workflows. When a health post currently using falciparum-only RDTs transitions to a p.f/p.v tri-line test, the change affects more than just the diagnostic step — it changes the treatment algorithm, the patient counseling protocol, and the case reporting system. Healthcare workers must be trained to interpret three test lines instead of two, distinguish between P. falciparum-positive-only results, P. vivax-positive-only results, mixed infections (both lines positive), and pan-Plasmodium-positive species-indeterminate results. The treatment decision for each scenario is different, and the training materials must cover each one. Manufacturers who provide clear, field-tested training aids — laminated reference cards with illustrated result interpretation guides — are better positioned for successful product adoption in public health programs than those who supply only a product IFU and leave the training to the distributor. The training requirement becomes particularly important when transitioning a national malaria program from falciparum-only RDTs to p.f/p.v tri-line tests, because healthcare workers who have been using two-line tests for years need to adapt to interpreting three-line results. Our training package for the Testsealabs tri-line malaria test includes a laminated quick-reference card, an instructional poster, and an IFU with illustrated result interpretation examples, all designed for use in health post settings.
One concern distributors raise about triplet-line RDTs in the African context is whether the additional capture and detection antibodies required for three test lines affect heat stability compared to simpler single-band formats. The manufacturing answer depends on the antibody sourcing and formulation process.
At Testsealabs, our p.f/p.v tri-line cassettes are manufactured using monoclonal antibodies sourced from established bioreactor-based production lines, not ascites fluid. The cassettes are formulated with stabilizers that protect antibody activity across the full 4–30°C storage range. Accelerated stability testing at 40°C demonstrates that all three test lines maintain their signal intensity within acceptable limits for the product’s two-year shelf life. For distributors supplying malaria RDTs to West Africa — where ambient temperatures routinely exceed 35°C for extended periods — this heat stability profile is a product differentiator worth evaluating.
Malaria remains the most significant parasitic disease in sub-Saharan Africa, but the diagnostic response must evolve to match the epidemiological reality. The evidence from molecular surveillance across multiple African regions makes it increasingly difficult to justify a procurement strategy based on falciparum-only RDTs in settings where P. vivax is circulating at clinically relevant levels. For distributors and ministries of health evaluating their malaria RDT procurement strategy, the transition from single-species to dual-species testing is not a matter of if, but when.
Conclusion
P. vivax is Africa’s underdiagnosed malaria species. Its prevalence across the continent is higher than most procurement data suggests, the clinical consequences of missing it are significant — both for individual patient outcomes and for malaria control programs — and the current procurement paradigm of falciparum-only RDTs is systematically underdiagnosing it. For distributors serving the African market, adding a quality-assured p.f/p.v tri-line RDT to the product portfolio addresses this diagnostic gap while creating commercial differentiation in a commoditized market.
Testsealabs’ Malaria p.f/p.v Tri-Line Test Cassette delivers species-level differentiation in a room-temperature-stable, 15-minute format backed by ISO 13485 manufacturing quality. If you are a distributor evaluating your malaria RDT portfolio and interested in addressing the P. vivax diagnostic gap, I welcome the opportunity to discuss how our products can support your public health procurement partners.
For authoritative guidance on malaria diagnostics and species-specific testing, I recommend reviewing the WHO Global Malaria Programme’s resources at WHO Global Malaria Programme.
About the Author
Angela Qin is the International Sales Director at Hangzhou Testsea Biotechnology Co., Ltd. (Testsealabs), with 10+ years of experience in the IVD industry. Testsealabs is an ISO 13485 and MDSAP-certified manufacturer of rapid diagnostic products covering infectious diseases including malaria, dengue, HIV, and respiratory infections. The company’s tri-line p.f/p.v malaria test is CE-marked, room-temperature stable, and manufactured in a 56,000-square-meter ISO 13485 facility serving over 100 countries.
Email: info@testsealabs.com
YouTube: Testsealabs
Facebook: Testsealabs on Facebook
Post time: Jun-25-2026